
Shoulder Arthritis
Shoulder Arthritis
What is Arthritis?
Arthritis is the degenerative damage that occurs to the cartilage surfaces of a joint. Cartilage is the tissue that makes the smooth surfaces of a joint. Cartilage allows for the smooth motion of the body’s joints. Arthritis can develop in a joint for a variety of reasons. Based cause of development, arthritis is categorized into different categories:
Degenerative Arthritis (aka Osteoarthritis)
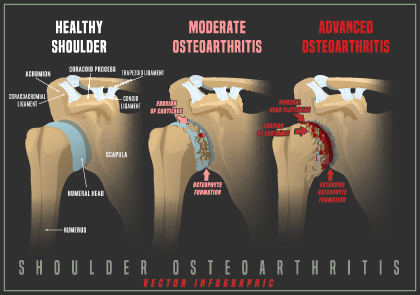
This is the most common cause of arthritis of joints. It is due to the natural changes associated with age. As we age, the cartilage of our joints undergoes cellular level changes that lead to weakening of the integrity of the cartilage. As the cartilage weakens, it begins to deteriorate and thin. Eventually, the cartilage exposes the underlying bone which accelerates the degeneration of the cartilage. By and large, everyone will experience this kind of change in every joint to some degree. Why certain joints in a person degenerate more extensively than others are not well understood. Nor do we understand why some individuals develop pain associated with arthritis while others do not. Osteoarthritis can by monoarticular (involving one joint) or polyarticular (multiple joints). Often there is symmetry with regards to joint involvement; in other words, if one shoulder is affected, then there is a higher probability that the other shoulder will also be affected. However, just because there may be symmetry in involvement, it does not mean that the right and left shoulder will be equally affected. The following article is a good resource for discussion about osteoarthritis: https://www.ncbi.nlm.nih.gov/books/NBK482326/
Inflammatory Arthritis
These kinds of arthritis are generally associated with an underlying autoimmune disease. Autoimmune inflammatory arthropathies constitute several conditions in which the body’s own immune system incorrectly identifies the joint tissues as foreign materials. This false recognition leads the body to create an immune response to the joint tissues. The immune response is akin to fighting off an infection type process. The body’s immune cells begin to “attack” the joint tissues and cause an inflammatory, painful response in the affected joints. The joint cartilage begins to deteriorate due to the inflammatory response of the body. The destructive changes to the joint and cartilage are often more rapidly than what is seen in osteoarthritic conditions. Associated soft tissue damage is often found in inflammatory arthritis conditions. For instance, in the shoulder, there is often associated rotator cuff damage with the joint damage. Inflammatory arthritis is often polyarticular (involves multiple joints) in nature. Examples of inflammatory arthritis include:
- Rheumatoid arthritis
- Lupus
- Irritable Bowel diseases
- Celiac Disease
- Psoriatic arthritis
- Gout
Early recognition and medical management are critical towards the prevention of progressive destructive arthritis of the joints of the body. Specialists known as Rheumatologists help patients control the body’s autoimmune destructive response to joints. The advances in medical management have helped patients protect and preserve their joints and avoid premature surgery. Unfortunately, though the disease process can be slowed down, the process continues and can eventually lead to joint damage that ultimately requires surgical intervention. In many instances, surgical intervention can be recommended to prevent progressive destructive changes that may make joint reconstruction difficult at a later stage.
The following article is a good resource for a discussion about inflammatory arthritis: https://www.ncbi.nlm.nih.gov/books/NBK507704/
Traumatic Arthritis
Arthritis that develops some time after an injury to a joint is categorized as traumatic arthritis. The severity of the joint injury often correlates with how quickly joint arthritis might progress: the more severe the joint injury, the more likely arthritis will occur sooner rather than later. For example, first time anterior shoulder dislocation injuries have been reported to have up to 50% incidence of development of arthritis (Hovelius L, Saeboe M. Neer award 2008: arthropathy after primary anterior shoulder dislocation—223 shoulders prospectively followed up for twenty-five years. J Shoulder Elbow Surg. 2009;18(3):339–347). Fractures involving the joint surface that result in a “step-off” of the surface have shown an increased risk of developing arthritis in the affected joint. (Giannoudis PV, Tzioupis C, Papathanassopoulos A, et al. Articular step-off and risk of post-traumatic osteoarthritis. Evidence today. Injury. 2010;41:986–995). For that reason, surgery is often recommended to restore congruency of the joint; all in an effort to reduce the risk of development of arthritis of the joint. Traumatic arthritis can develop after joint dislocations, fractures, prolonged repetitive strenuous activities over the course of years (such as seen in competitive body builders).
The following article is a good resource for a discussion about traumatic arthritis:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5013366/
Septic Arthritis
Arthritis can develop after a joint develops and recovers from a bacterial or viral infection. Joint infections can occur due to seeding of the pathogen from a blood infection due to another cause such as Lyme disease and certain types of viral diseases. Infection can come from a traumatic inoculation of the joint due to an injury. An example of this could be an animal bite or a penetrating injury such as a thorn, knife, or gun shot. Septic arthritis issues are considered surgical emergencies. Treatment with long term antibiotics is often necessary. Even with appropriate treatment, the cartilage of the joint is often damaged due to the infection such that future arthritis is a likely outcome for the affected joint. The severity of arthritis that develops in the joint is often related to the severity of the infection in the joint.
Avascular Necrosis
This is a painful disorder in which the blood supply to an affected bone near a joint loses its blood supply. The loss of blood flow to the bone causes bone death. Often the bone death occurs near the joint surface. The dying bone collapses causing a deformity of the joint surface. The adjacent cartilage can break off the dead bone and becomes what is known as a loose body inside of the joint. The loose body can cause mechanical symptoms of locking and catching of the joint with motion. The deformity of the bone eventually causes the development of arthritis of the joint due to mechanical grinding. When identified early, avascular necrosis can be treated with procedures to restore blood flow to the affected bone. After joint collapse and/or cartilage loss, surgical procedures are directed towards correcting deformity and restoring joint congruency. Causes of avascular necrosis include trauma, use of steroids (often after a short high dose use or after prolonged long-term use), and excessive alcohol use. Avascular necrosis can also be idiopathic, meaning that an obvious cause is never identified.
Shoulder Arthritis
Any of the types of arthritis discussed can afflict the shoulder joint. There are two shoulder joints that can develop arthritis: the acromioclavicular joint and the glenohumeral joint.
Acromioclavicular arthritis
The acromioclavicular joint is the joint made up by the acromion bone of the scapula and the lateral end of the clavicle. AC joint degeneration is most associated with osteoarthritis and traumatic arthritis etiologies. A condition known as distal clavicle osteolysis is associated with repetitive heavy weightlifting activities such as body building exercises. Distal clavicle osteolysis is akin to an avascular necrosis pathology in that there is structural bone loss to the distal clavicle. Most individuals will develop some form of osteoarthritis in the acromioclavicular joint with age. Symptomatic arthritis of the acromioclavicular joint does not necessarily correlate with x-ray findings of arthritis. Initial treatment for symptomatic acromioclavicular arthritis is generally conservative. Nonsurgical treatments include the use of NSAIDs, ice, KT taping, rest, modification of activities, and cortisone injections. For failed conservative treatment, definitive surgical treatment can be performed. Surgery can be done arthroscopically or via a mini-open procedure.
Glenohumeral Arthritis
Arthritis of the ball and socket joint of the shoulder is known as glenohumeral arthritis. The glenohumeral joint is the ball and socket joint of the shoulder which allows an individual to place the arm almost any position in space away from the body. As with any other major joint, glenohumeral arthritis can develop from any of the etiologies described previously.
For the shoulder, glenohumeral arthritis can further be broken down into 2 additional categories:
- Arthritis with an INTACT rotator cuff
- Rotator cuff tear arthritis
Both forms of glenohumeral arthritis can develop from osteoarthritis, inflammatory arthritis, avascular necrosis, septic arthritis, and traumatic arthritis. The important differentiation of the 2 types of shoulder arthritis pathologies has to do with the integrity of the rotator cuff and how that rotator cuff integrity determines the type of shoulder replacement can be considered for shoulder reconstruction surgery.
The treatment for shoulder glenohumeral arthritis is catered to the individual patient and should take into consideration the goals, expectations, and life requirements for the patient. Initial nonsurgical treatment is usually the first appropriate step for acute onset pain with preserved shoulder function and non-destructive radiographic findings. Conservative treatments include the use of anti-inflammatory medications, modalities such as ice and heat, physical therapy focused on pain relief and restoration of motion, and steroid injections.
Surgical intervention shoulder glenohumeral arthritis is generally reserved for individuals who fail to respond to conservative treatment and/or suffer from severe functional range of motion limitations due to deformity and/or progressive destructive changes that could prohibit shoulder replacement surgery in the future.
For “young patients” with mild shoulder glenohumeral arthritis with an intact rotator cuff and no deformities of the humeral head or glenoid, surgical options include arthroscopic debridement known as a CAM procedure (comprehensive arthroscopic management). The CAM procedure involves several sub procedures, all of which are done arthroscopically:
- Glenohumeral debridement
- Chondroplasty
- Removal of loose bodies
- Synovectomy
- Humeral osteoplasty
- Capsular release
- Axillary nerve Neurolysis
- Additional
- Acromioplasty/Bursectomy
- Coracoplasty
- Biceps Tenodesis
For “older patients” and/or patients who present with more advanced glenohumeral joint arthritis findings that include deformities of the humeral head and/or glenoid, and/or associated rotator cuff tears, total shoulder joint replacement becomes the most reliable option for pain relief and restoration of function to the shoulder.
For patients who fall into this category of glenohumeral arthritis who have an intact and healthy rotator cuff, the surgery of choice is an anatomic total shoulder replacement procedure. As the name suggests, an anatomic shoulder replacement replaces the arthritic humeral head and glenoid surfaces with a prosthetic metal ball and a specially fabricated polyethylene socket component respectively. An anatomic shoulder replacement mandates a functional and healthy rotator cuff is present.
For patients who also have a deficient, damaged, poor quality rotator cuff in the setting of glenohumeral arthritis, the surgery of choice is a reverse total shoulder arthroplasty. As the name suggests, a reverse shoulder replacement “reverses” the configuration of the ball and socket components as they relate to the “normal” glenohumeral joint configuration. In other words, the ball component, called the glenosphere, is placed onto the glenoid (socket) and the cup component is placed onto the arm bone where the native ball used to be. The reverse shoulder replacement bypasses the dysfunctional and damaged rotator cuff. It uses the large deltoid muscle to help the arm regain the ability to reach and function overhead. Therefore, an intact deltoid muscle is necessary to successfully perform a reverse shoulder replacement.
Emerging Treatments for Glenohumeral Arthritis
There are several emerging biologic treatments for shoulder glenohumeral arthritis that are finding their way into mainstream application. Of these emerging technologies, a biologic treatment known as PRP has gained some traction in the treatment of musculoskeletal injury and disease. PRP stands for platelet rich plasma. At its essence, it is comprised of the growth factors derived from a person’s blood and/or bone marrow. This technology is being increasingly used to “biologically” enhance the healing potential of soft tissue injuries and surgical repairs of the musculoskeletal system. There has been some gaining interest in the use of PRP as an alternative to the use of steroid injections to treat early arthritis in various joints. The philosophy behind the interest in the use of PRP as an alternative to steroid injections comes from the growing evidence that steroid injections into joints can accelerate arthritic damage in a given joint; thereby pushing the patient further down the path towards joint replacement surgery faster. Further evidence-based research is needed to quantify PRP as a valuable tool in the treatment of glenohumeral joint arthritis. However, in the setting of limited options for a young patient with mild osteoarthritis who is not responding to medical management, it may serve as a less caustic option to the glenohumeral joint than repetitive steroid injections.
Consult a Shoulder Surgeon in Boise
Whether you’ve already been diagnosed with shoulder arthritis or you’ve been living with unexplained shoulder pain and functional limitations for too long, our orthopedic shoulder fellowship trained surgeon can help.
