
Fractures of the Humerus
Fractures of the Humerus
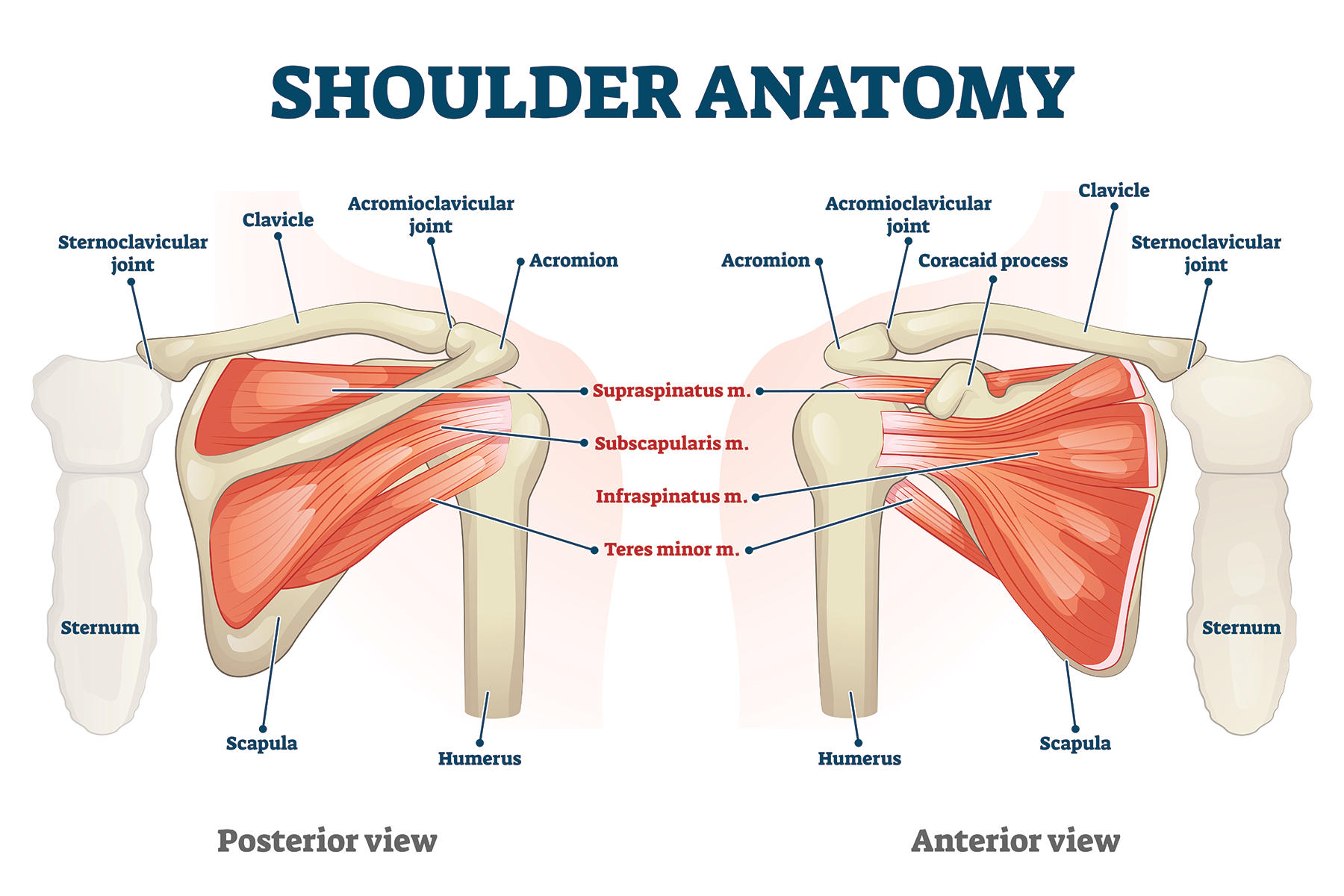
The arm bone is called the humerus. The upper part of the humerus is called the proximal humerus. The proximal humerus forms the ball of the shoulder joint. The proximal humerus has certain bony landmarks to which important soft tissue structures attach. 2 of those bony landmarks are known as the greater and lesser tuberosities. The posterior and superior rotator cuff tendons (Supraspinatus, Infraspinatus, and Teres Minor) attach to the greater tuberosity. The anterior rotator cuff tendon (Subscapularis) attaches to the lesser tuberosity. In between the tuberosities, there is a groove known as the bicipital groove. The long head of the biceps runs through this groove into the shoulder joint to attach onto the superior glenoid rim by way of the superior labrum.
The humeral head region is divided into 2 zones known as the anatomic neck and surgical neck. The anatomic neck encompasses the true articular surface of the humeral head. The surgical neck encompasses the zone of the proximal humerus where fractures often occur. The zones are important as they can differentiate the viability of the humeral head when a proximal humerus fracture occurs.
Proximal humerus fractures occur at or above the surgical neck. Fractures are designated by various classifications but the most clinically used classification is the Neer classification. Dr. Neer classified proximal humerus fractures into 4 categories based upon which structure(s) were involved in the fracture (humerus shaft, surgical neck, anatomic neck, greater tuberosity, lesser tuberosity). The fractures are classified based on how the parts are oriented in relation to each other and how they are oriented in relation to the humerus shaft.
1 Part Fracture:
One-part fractures involve either the surgical neck, anatomic neck, lesser tuberosity, or greater tuberosity. These fractures have less than 1 cm of displacement and are usually treated non-surgically.
2 Part Fracture:
Two-part fractures involve the surgical neck, anatomic neck, lesser tuberosity, or greater tuberosity and demonstrate 1 or more centimeters of displacement. These may or may not need surgical treatment based upon which part of the proximal humerus is fractured, how much displacement is present, and in which direction the displacement has occurred.
3 Part Fracture:
Three-part fractures involve the surgical neck and greater tuberosity or surgical neck and lesser tuberosity. The fragments are displaced from each other by at least 1 centimeter. 3-part fractures often require surgery.
4 Part Fracture:
Four-part fractures involve the surgical neck (often includes the anatomic neck), the lesser tuberosity, and the greater tuberosity. The fragments are displaced from each other by at least 1 centimeter. 4-part fractures require surgery.
Non-Surgical Treatment
Non-surgical treatment is indicated for non-displaced 1 part and minimally displaced 2-part fractures. Sling immobilization is the mainstay of treatment. The sling is worn until x-ray signs of healing are present. Once x-rays show interval healing of the fracture, formal physical therapy is initiated to regain motion and function. Strengthening is initiated when adequate x-ray healing has occurred and pain is minimal. Recovery can take anywhere from 12-16 weeks to regain functional abilities overhead with the arm. Full “normal” return to function can take 16-24 weeks.
Surgical Treatment
Displaced 2-part, most 3-part, and nearly all 4-part fractures will require surgery to restore shoulder function. Surgery falls into 2 possible options: Open reduction and internal fixation (ORIF) or shoulder replacement.
ORIF is performed by applying a specially made plate and screws to the fracture to internally stabilize the fragments. An alternative method of ORIF is by applying an intra-medullary nail into the bone to stabilize the fracture. Bone quality is a key factor in achieving success with. Both methods have their indications as well as pros and cons. ORIF is performed for displaced 2-part fracture. 3-part fractures in young people and those fractures that have preserved blood supply to the anatomic neck are treated with ORIF.
When the articular head (the anatomic neck) loses its blood supply and/or the bone quality is very poor, shoulder replacement becomes the surgery of choice to restore shoulder function.
Shoulder Replacement for Proximal Humerus Fractures
3-part fractures with blood loss to the anatomic neck, 3-part fractures with poor bone quality in elderly or unhealthy patients, and 4-part fractures benefit from shoulder replacement surgery to restore shoulder function.
Shoulder replacement has 2 options: hemiarthroplasty or reverse total shoulder arthroplasty.
Hemiarthroplasty
Shoulder hemiarthroplasty is a procedure in which the fractured proximal humerus is replaced by a ball and stem component to restore shoulder function. Functional recovery is dependent upon the healing of the greater and lesser tuberosities and the associated rotator cuff tendons to which it is attached. Without a good rotator cuff, a hemiarthroplasty should not be performed as the shoulder will not achieve good functional overhead motion and use. Similarly, the greater and lesser tuberosities have to be of adequate structural integrity with good bone quality for them to heal to the hemiarthroplasty construct.
Shoulder hemiarthroplasty is most performed in severe fractures in young active people who have good bone quality in which the fracture cannot be fixed. Other indications for hemiarthroplasty involve elderly people who are at risk of possible dislocations of a reverse total shoulder arthroplasty due to a falls risk, unreasonable weightbearing needs (such as for transfers or wheelchair bound individuals), and poor ability to comply with rehabilitation protocols.
Reverse Total Shoulder Arthroplasty (RTSA)
Reverse total shoulder arthroplasty has become the standard of care for proximal humerus fractures that cannot be repaired in the elderly population or population whose bone quality is of very poor quality. RTSA has improved the outcomes of function for patients who experience complex proximal humerus fractures that otherwise cannot be repaired.
Though the greater and lesser tuberosity healing are not essential to functional recovery with a reverse total shoulder arthroplasty for fracture, healing of the tuberosities most certainly improves functional recovery and strength. Healing of the greater tuberosity is important to restore the ability to externally rotate the shoulder so that one can reach the back of one’s head. If the greater tuberosity does not heal, there is a increased risk of a less than optimal outcome of shoulder function recovery. Patients who do not heal their greater tuberosity often develop what is known as a “Hornblower’s sign.” This functional impairment is when the patient cannot externally rotate the arm.
Healing of the lesser tuberosity is less critical in the successful functional outcome of a reverse shoulder replacement. However, healing of the lesser tuberosity is believed to improve the stability of the reverse shoulder replacement and reduce the risk of dislocation of the prosthesis.
Recovery from reverse total shoulder replacement for fracture of the proximal humerus is lengthier than that of a reverse total shoulder replacement for arthritis. Generally, a limited therapy program to move the shoulder is begun 2 weeks after surgery to promote early motion and prevent stiffness. As every effort is made to ensure that the greater tuberosity heals to improve functional use with external rotation, therapy is a much more deliberate and slower process for fracture arthroplasty. Once x-rays verify good healing of the greater tuberosity, a more aggressive therapy program is initiated to maximize motion and regain strength.
Reverse shoulder replacements for proximal humerus fractures are successful at recovering overhead functional range of motion to the shoulder. Often, there is some residual stiffness in every direction of motion due in part to the fracture and secondary injuries to soft tissues and partly due to the slower rehabilitation to ensure tuberosity healing.
Humeral Shaft Fractures
Humerus shaft fractures below the surgical neck and above the elbow joint articulation region are classified as humeral shaft fractures. Treatment for humerus shaft fractures depend upon several factors. These factors include orientation of the fracture, displacement, comminution, shortening, associated fractures in other areas due to trauma, presence of a radial nerve injury, and whether the fracture is open (exposure to air due to disruption of the skin).
Closed, minimally displaced or reducible non-transverse fractures in the middle of the humerus can be treated with a fracture brace (known as a Sarmiento Brace). Fracture brace treatment requires full time bracing and protection to allow the fracture to heal. Generally, it takes anywhere from 8 to 10 weeks for adequate healing to occur so that the patient can begin to gently use the arm for light activities. Bracing is worn until there is adequate x-ray findings of bone healing such that concern for re-fracture is no longer present. Restrictions in use or motion of the arm are maintained until the fracture shows adequate signs of healing on x-rays. Complications from non-surgical healing include nonunion (bone does not heal), malunion (bone heals crooked), and the development of shoulder stiffness (frozen shoulder).
Surgical Treatment
Surgical treatment of humeral shaft fractures is known as open reduction and internal fixation (ORIF). ORIF can be performed either via application of a plate and screw construct to stabilize the fracture or via an intramedullary nail. Both procedures have their indications and pros and cons. The benefits of surgical intervention include anatomic reduction of the fracture, early ability to mobilize the extremity for light use of activities of daily living (within 2 weeks of surgery), and shorter duration of acute pain as the fracture will have been stabilized.
The biggest risk of surgical intervention involves possible injury to the radial nerve due to its location against the humerus. Direct injury to the nerve is generally avoidable with ORIF. There is a slightly increased risk of radial nerve entrapment in the fracture with intramedullary nailing.
Unfortunately, a transient radial nerve palsy can occur due to fracture manipulation and soft tissue retraction during surgery. It can just as easily occur due to displacement of the fracture at the time of injury. A transient nerve palsy is when a nerve “falls asleep” for a limited period of time. In the case of a radial nerve palsy, the result is a loss of the ability to extend the wrist and extend the fingers or thumb for a duration of time. Transient radial nerve palsies generally resolve in anywhere from 6 to 12 weeks. If after 6 weeks there is still absolutely no nerve recovery, exploration of the nerve is often recommended to evaluate its integrity and status.
