
Shoulder Impingement Syndrome
Shoulder Impingement Syndrome
Anatomy and Function of the Shoulder
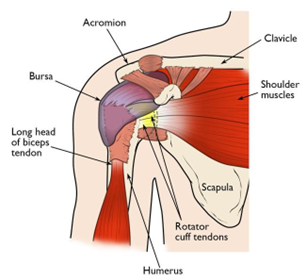 The shoulder joint is a ball and socket joint that connects the bone of the upper arm (humerus) with the shoulder blade (scapula). The shoulder joint is moved and stabilized by the rotator cuff. The rotator cuff is comprised of 4 muscles and their tendons that attach from the scapula to the humerus. The rotator cuff tendons (subscapularis supraspinatus, infraspinatus, and teres minor) cover the shoulder joint and capsule from front, over the top, and around the back. The muscles of the rotator cuff help stabilize the shoulder and enable you to lift your arm, reach overhead, and take part in activities such as throwing, swimming, and other sports such as tennis. To lubricate and protect the rotator cuff, a bursal sac covers the rotator cuff in the subacromial space. The subacromial space is the space through which the rotator cuff slides as the arm is raised, abducted, and elevated. The roof of the subacromial space is the acromion. The floor of the subacromial space is the humeral head. There is some evidence indicating the bursal sac may provide some nutritional support to the rotator cuff tendons. The bursal sac promotes smooth gliding of the rotator cuff through the subacromial space when the arm is abducted, elevated, and the shoulder is rotated.
The shoulder joint is a ball and socket joint that connects the bone of the upper arm (humerus) with the shoulder blade (scapula). The shoulder joint is moved and stabilized by the rotator cuff. The rotator cuff is comprised of 4 muscles and their tendons that attach from the scapula to the humerus. The rotator cuff tendons (subscapularis supraspinatus, infraspinatus, and teres minor) cover the shoulder joint and capsule from front, over the top, and around the back. The muscles of the rotator cuff help stabilize the shoulder and enable you to lift your arm, reach overhead, and take part in activities such as throwing, swimming, and other sports such as tennis. To lubricate and protect the rotator cuff, a bursal sac covers the rotator cuff in the subacromial space. The subacromial space is the space through which the rotator cuff slides as the arm is raised, abducted, and elevated. The roof of the subacromial space is the acromion. The floor of the subacromial space is the humeral head. There is some evidence indicating the bursal sac may provide some nutritional support to the rotator cuff tendons. The bursal sac promotes smooth gliding of the rotator cuff through the subacromial space when the arm is abducted, elevated, and the shoulder is rotated.
What is Shoulder Impingement
Shoulder impingement is a condition in which the rotator cuff tendons and subacromial bursa pinch against the undersurface of the acromion as the arm is lifted into abduction and/or elevation for overhead positions. The pinching prevents normal sliding of the rotator cuff tendons and bursa. The rotator tendons and subacromial bursa become progressively irritated and inflamed. The irritation and inflammation lead to swelling of the rotator cuff and bursa. The swelling worsens the impingement thus creating a vicious cycle. Eventually, a bone spur can form on the undersurface of the acromion causing the subacromial space to narrow thereby worsening the shoulder impingement.
Shoulder impingement has also been called by other names including:
- Rotator cuff Tendinitis
- Shoulder Bursitis
- Rotator cuff Impingement
- Subacromial Bursitis
- Subacromial Impingement
Diagnosis Shoulder Impingement
Shoulder impingement can develop due to repetitive shoulder activities. Sports such as swimming, tennis, pickleball, baseball, football and other throwing or racket sports. Repetitive or prolonged overhead work activities can result in shoulder impingement. Shoulder trauma or injury can lead to shoulder impingement. Conditions causing shoulder stiffness such as frozen shoulder, also known as adhesive capsulitis, can result in a secondary shoulder impingement. Shoulder impingement can also develop as an insidious process.
Symptoms of shoulder impingement often include pain, loss of motion, stiffness, and weakness. Patients can report pain with sleep, especially when laying on the affected shoulder. Patients may complain of popping, grinding, grating, crunching in the shoulder with rotation and when raising the arm.
Examination of the shoulder usually reveals pain with motion above shoulder level. There is often tenderness along the lateral part of the shoulder. There may be a sense of warmth and swelling along the lateral shoulder. Pain can radiate down the lateral arm. Patients may experience a sense of shoulder weakness due to the pain.
The diagnosis can often be confirmed by history and examination. Occasionally, an MRI can be done for cases that do not get better with conservative measures or for severe cases at presentation
Differential Diagnosis for Impingement Syndrome
There are several other conditions that can mimic impingement syndrome. These include:
- Calcific tendinitis
- Rotator cuff tears
- Frozen Shoulder (Adhesive Capsulitis)
- Acromioclavicular arthritis
Most of these conditions can be differentiated by x-rays, examination, and MRIs.
Treatment of Shoulder Impingement
Treatment generally starts with conservative measures.
The treatment selected often depends on the level of pain and duration of symptoms that the patient has at the time of evaluation.
For mild symptoms and those present for a short duration of time (less than 6 weeks), a course of home exercises, modification of activity, rest, modalities such as ice and heat, and use of nonsteroidal anti-inflammatories is recommended.
For more severe symptoms and those present for a longer duration of time (greater than 6 weeks), consideration can be given to try a cortisone (steroid) injection into the subacromial space (the space between the rotator cuff and acromion where the subacromial bursa is located). After the acute pain resolves, further treatment with home exercises, modification of activity, rest, modalities of ice and heat, and nonsteroidal anti-inflammatories are instituted.
Physical therapy may be recommended when the patient presents with loss of motion, loss of strength, or if the patient does not respond to conservative measures.
For symptoms not responding to conservative measures, an MRI may be considered to look for other causes of shoulder pain.
Surgical Treatment for Shoulder Impingement
Surgery for Impingement syndrome is usually a last resort treatment for failed conservative treatment. Surgery is generally an arthroscopic procedure called a subacromial decompression and acromioplasty. A subacromial decompression is a procedure in which the irritated and inflamed subacromial bursa is removed to allow healthy bursa to grow back in its place. An acromioplasty is when an overgrown bone spur that develops on the undersurface of the acromion is shaved away to create more space in the subacromial space. Often both procedures are performed simultaneously.
Post-surgical recovery generally takes anywhere from 10-12 weeks for full recovery. Recovery is a progressive program of early range of motion and light daily use allowed within 2 weeks after surgery. Within 4-6 weeks after surgery, most patients are allowed to increase their activities as tolerated. Post-surgical physical therapy can often be initiated as a progressive home program. Formal physical therapy can be initiated for patients having difficulty with recovery of motion and use with home exercises alone.
Subacromial decompression and acromioplasty procedures are often performed in association with rotator cuff repair surgeries.
Factors Affecting Healing and Outcomes after Surgery
Many factors determine the healing and end outcome of surgical repair after rotator cuff tear. These factors include:
- Age of patient
- Associated findings of rotator cuff degenerative tendinopathy
- Quality of the Rotator cuff tendon
- Medical Co-morbidities: Diabetes, Obesity, Kidney disease, Liver disease, etc.
- Smoking
