
Carpal Tunnel Syndrome
Carpal Tunnel Syndrome
Carpal Tunnel Syndrome is a very common condition that affects the hand and wrist. Symptoms may include pain, numbness and tingling, finger stiffness, loss of dexterity, grip and pinch strength loss, and radiating pains up from the wrist into the forearm; occasionally up to the shoulder.
The condition occurs as one of the major nerves of the hand – median nerve – is compressed and squeezed as it travels through the wrist into the hand.
In most patients, carpal tunnel syndrome will progress over time. Therefore, early diagnosis and treatment are important. Progressive symptoms that are ignored can lead to chronic irreversible nerve damage, muscle weakness and atrophy, and chronic pain.
When diagnosed early, simple treatments such as wearing splints, modifying activities, ergonomic work adjustments, and use of anti-inflammatory medications may relieve symptoms. The use of cortisone injections and/or oral steroid medications in some instances may help reduce acutely severe symptoms.
If symptoms continue or progressively worsen over time, then surgery is often recommended to prevent permanent nerve damage. The purpose of surgery is to remove the pressure on the median nerve and prevent worsening damage to the nerve. The added benefit in most patients is significant resolution of their symptoms.
Anatomy
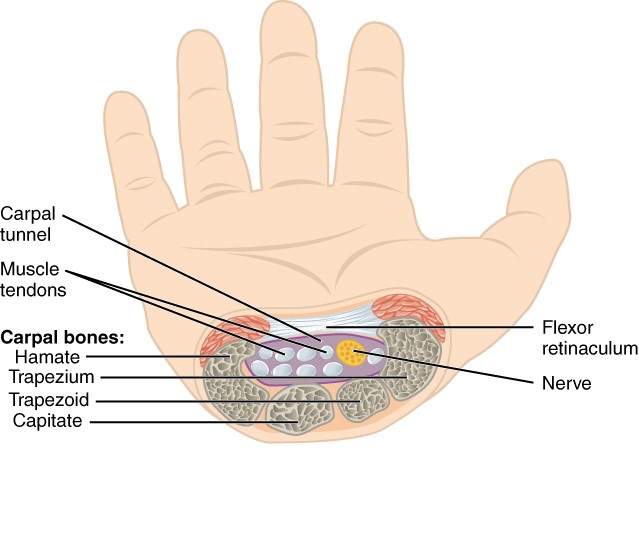 The carpal tunnel is a narrow passageway in the wrist and hand. The floor of the tunnel and sides of the tunnel are formed by the small wrist bones called the carpus. The roof of the tunnel is a strong, rigid band of tissue called the transverse carpal ligament. These structures form a rigid, fixed space which has no capacity to expand or “stretch”.
The carpal tunnel is a narrow passageway in the wrist and hand. The floor of the tunnel and sides of the tunnel are formed by the small wrist bones called the carpus. The roof of the tunnel is a strong, rigid band of tissue called the transverse carpal ligament. These structures form a rigid, fixed space which has no capacity to expand or “stretch”.
The median nerve is one of the 2 mains nerves to the hand. It originates from a group of nerves roots in the neck. These roots come together to form the median nerve which travels down through the arm, forearm, through the carpal tunnel, to end in the hand and fingers. The nerve branches in the hand to generally provide sensation to the thumb, index, and middle fingers. A branch of the nerve also controls a group of muscles at the base of the thumb.
In addition to the median nerve, the nine flexor tendons that bend the fingers and the thumb also travel through the carpal tunnel.
Causes of Carpal Tunnel Syndrome
Carpal tunnel syndrome is likely caused by a combination of factors both medical and environmental. Studies have shown that women and advanced age individuals are more likely to develop the condition. Risk factors include:
- Medical disease
- Diabetes, Inflammatory arthritis, Thyroid Disease, Hepatitis, HIV, Renal Disease
- Transient Medical Conditions
- Pregnancy, Cancer treatments
- Masses, cysts, tumors, accessory muscles
- Fractures, sprains, and ligament injuries to the wrist
- Altered anatomy due to old injuries
- Genetics
- Idiopathic – No identifiable cause
Repetitive use activities are thought more to aggravate the symptoms of carpal tunnel syndrome rather than be a primary causative factor for the development of carpal tunnel syndrome.
Symptoms
Symptoms of carpal tunnel syndrome include:
- Numbness, tingling, burning sensations, and pain
- Primarily involves the thumb, index, middle, and ring fingers
- Radiation of symptoms into the forearm and up the arm
- Weakness and clumsiness in the hand
- Loss of dexterity activities such as buttoning, picking up small objects
- Dropping objects
- Due to weakness, numbness, or loss of proprioception (spatial awareness of the hand)
In most cases, the symptoms of carpal tunnel begin gradually, without specific injury, and gradually worsen over time. At first, symptoms may wax and wane. Over time, symptoms may become more severe, frequent, and constant.
Nighttime symptoms are very common, often disturbing restful sleep. Daytime symptoms may be exacerbated by daily life activities such as driving, writing, typing, reading a book, or using an electronic device such as a phone, tablet, or laptop.
Many individuals find that they must “shake” the hand to relieve the symptoms.
Diagnosis and Testing
Health assessment and medical history are integral in determining medical, environmental, and exposure related factors contributing to the diagnosis of carpal tunnel syndrome. In addition, a thorough examination of both upper extremities and cervical spine will usually be performed by your treating physician.
Testing may include one or more of the following:
- X-rays
- Provides evaluation of the bones of the wrist and hand to better appreciate the architecture of the joints of the wrist and hand. Allows your physician to rule out arthritis, ligament injuries, bone tumors, and abnormal calcifications.
- Nerve Conduction Studies and Electromyography
- These test help to verify the presence of carpal tunnel syndrome and quantify the severity of carpal tunnel syndrome. Often the study is performed on both the affected upper extremity and the unaffected extremity to provide a good comparison study for each individual. Occasionally, a lower extremity may be tested to provide further nerve function data to rule out other nerve diseases.
- MRI
- Though not routinely performed, this study may be ordered when there is concern for masses, tumors, or other abnormal tissue that may be present in the carpal tunnel.
Treatment
For most individuals, the symptoms of carpal tunnel syndrome will gradually worsen over time. In its early stages, it may be possible to slow or “stop” the progression of the condition.
Nonsurgical Treatment:
If diagnosed and treated early, the symptoms of carpal tunnel may often be treated without surgery. Nonsurgical treatments may include one or more of the following:
- Bracing or Splinting
- Wearing a brace or splint at night will keep your wrist from positions that may aggravate pressure upon the median nerve in the carpal tunnel. Daytime use is generally recommended for activities that aggravate the carpal tunnel symptoms. The splint should not be worn continuously during awake hours.
- Non-steroidal anti-inflammatories
- Medications such as ibuprofen and naproxen may help calm inflammation and reduce tissue swelling. Long term use of such medications should be discussed with one’s primary care physician for safety and medication interactions.
- Activity change
- When possible, avoid prolonged wrist positions which may aggravate symptoms. In many instances, workstation adjustments (ergonomic) can be very helpful to reduce symptoms.
- Exercises
- Nerve Glide Exercises may be recommended to promote the median nerve to move more freely within the confines of the carpal tunnel.
- Steroid Medications
- Steroid medications can be prescribed orally or via a local injection provided into the carpal tunnel. Corticosteroid is a powerful anti-inflammatory agent. Generally, a corticosteroid injection will be more effective than oral steroid medications. Although these medications may relieve painful symptoms or help to calm a flare of symptoms, their effects are often temporary. In addition, repetitive use of steroids whether given orally or injected can have long term detrimental effects to tissue.
Surgical Treatment:
If nonsurgical treatment does not alleviate your symptoms or you have more advanced signs of carpal tunnel syndrome, surgical nerve decompression surgery may be recommended.
The decision whether to have surgery is based upon the severity of an individual’s symptoms in combination with the severity of the quantitative data obtained from the nerve conduction/EMG study. In chronic cases with advanced nerve damage and muscle damage, surgery may still be recommended to prevent worsening damage to the nerve.
Surgical Procedure
The surgical procedure performed for carpal tunnel syndrome is called a Carpal Tunnel Release. The goal of surgery is to relieve the pressure on the median nerve by cutting the ligament that forms the roof of the carpal tunnel. Transecting this ligament enlarges the tunnel and therefore decreases the pressure on the nerve.
Carpal tunnel surgery is performed as an outpatient surgery. The surgery is generally performed with intravenous sedation (“twilight”) combined with an injection of local anesthetic (lidocaine) around the surgery site.
Regardless of the surgical technique employed, the risks and outcomes of surgery are similar.
Recovery
The surgical procedure generally takes less than 20 minutes. A soft bandage will be applied to provide compression, support, and swelling control. This bandage is removed 24 hours after surgery and band aids are applied to the incision area.
Early finger motion is encouraged to prevent stiffness and swelling. In addition, frequent elevation and application of ice packs for the first 48-72 hours is recommended.
Finger soreness with motion, mild pain, swelling in the palm and fingers, mild bruising, and palm soreness should be expected for several weeks after surgery.
Symptoms of carpal tunnel syndrome generally resolve within 2-3 months after surgery. If the condition of the median nerve was poor prior to surgery (i.e. advanced stages), symptoms may not resolve for 6-12 months. It is generally accepted that if one continues to have symptoms after 6 months, then incomplete resolution of symptoms from surgery is to be expected.
Generally, splints or braces are not required after surgery. Light activities and daily life activities are generally allowed beginning the day after surgery. Driving, writing, typing, and other sedentary work activities are allowed as soon as one feels comfortable.
Return to work is dependent upon specific work requirements and accommodations that can be provided during the initial recovery.
Therapy is generally not required after surgery. Therapy may be utilized for significant surgical swelling or persistent palm or incisional pain. Therapy does not accelerate nerve recovery.
Complications
Complications are an unfortunate possibility with any surgery. Many steps are taken to minimize the risk of complications including obtaining appropriate medical clearance and blood work prior to surgery, and the administration of IV antibiotics at the time of surgery. The most common complications from carpal tunnel surgery include:
- Surgical site infection
- Generally, less than 1%
- There is a higher risk of infection in individuals with diabetes and medical conditions that reduce the strength of one’s immune system.
- Surgical site bleeding/bruising
- More common in patients who take blood thinning medications
- Transient Nerve symptom aggravation
- Nerve injury
- 2-5% of the population can have unusual nerve anatomy that may be injured during carpal tunnel release.
- Pillar Pain
- Prolonged or chronic pain at the site of ligament transection in the base of the palm that can occur after carpal tunnel release
Outcomes
Patient reported success rates for carpal tunnel surgery range from 75-95%. Most individuals report improvement in symptoms with carpal tunnel surgery. Recovery, however, may be gradual and take up to 1 year for maximum resolution of symptoms.
In general, most individuals report quicker resolution of night symptoms within weeks of surgical release. Daytime symptoms, hand weakness, and clumsiness may take several months to resolve, as these symptoms are often associated with some element of nerve damage and ultimately may lead to incomplete resolution of symptoms.
Soreness about the surgical site is to be expected for anywhere from 6-12 weeks, gradually resolving with each week after surgery. If pillar pain develops after carpal tunnel release, it generally subsides over time with appropriate therapeutic exercises. There are instances where pillar pain becomes a chronic after effect of carpal tunnel release. The development of pillar pain after carpal tunnel surgery is an unpredictable phenomenon and is poorly understood at this time.
The likelihood of full recovery becomes less likely if symptoms persist beyond 6 months after surgical release; though less dramatic improvements can still be seen for up to 1 year post surgical release.
Chronic changes such as muscle-wasting and atrophy are permanent and will not resolve with carpal tunnel release. In addition, symptoms attributable to other orthopedic conditions such as arthritis or tendonitis, and neurologic diseases such as diabetic neuropathy and cervical spine arthritis will not be alleviated with carpal tunnel release.
Carpal tunnel release does not guarantee the ability to return to those activities which may have aggravated or played a role in the development of the disease process. Activities, work related or otherwise, that may lead to repetitive overuse injuries can re-aggravate or “flare up” carpal tunnel symptoms even after surgical release. Proper ergonomic positioning and appropriate modification of activities are critical to prevent recurrent symptoms. Despite such efforts, sometimes certain recreational activities and work activities may have to be avoided.
