
Acromioclavicular Joint
Arthritis of the Shoulder
Acromioclavicular Joint
Arthritis of the Shoulder
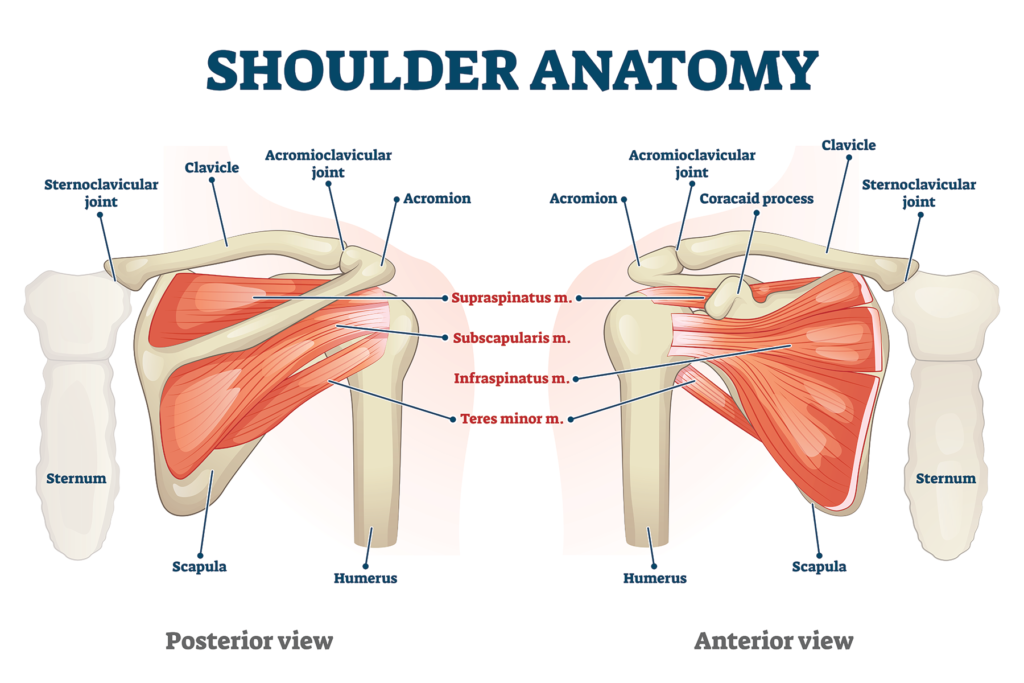
The AC joint is located at the tip of the shoulder where the shoulder blade (scapula) and collarbone (clavicle) come together at a point on the upper part of the shoulder blade called the acromion. These two bones are held together by ligaments. One group of ligaments envelope the joint to form a capsule that covers the joint; these ligaments are termed the acromioclavicular ligaments. Another set of ligaments stabilize the shoulder by holding the clavicle in place by attaching it to a bony projection on the surface of the shoulder blade called the coracoid process. These ligaments are called the coracoclavicular ligaments. There is a disk of cartilage in the joint between the two bones that help guide the joint movement. As you move your shoulder, the AC joint allows the movement to occur between the clavicle and scapula.
What is Acromioclavicular joint arthritis of the shoulder?
AC joint arthrosis, or osteoarthritis of the acromioclavicular joint is most common in people who are middle aged. It develops when the cartilage in the AC joint begins to wear out. With this condition, there is usually pain that limits the motion of the arm.
Causes of AC arthritis of the shoulder
The principal cause of AC joint arthritis is wear and tear due to use. As a person uses his/her arm and shoulder, stress is placed on the AC joint. This stress produces wear and tear on the cartilage, the cartilage becomes worn over time, and eventually arthritis of the joint may occur. Persons who must use their arms for extended periods of time are susceptible to AC joint arthrosis. Constant overhead lifting, such as is engaged in by weightlifters or construction workers who work overhead, can increase the incidence of the disease. Other susceptible individuals are athletes participating in contact sports or engaging in any activity that may result in a fall on the end of the shoulder.
Symptoms of AC arthritis of the shoulder
One of the first signs that a person may have arthrosis of the AC joint is pain and tenderness at the top of the shoulder around the joint. Sleeping on the side may cause pain. There may be a decrease in shoulder motion. Compression of the joint, such as bringing the arm across the may result in increased pain. There may be some swelling at the site of the joint. If the AC joint had been injured some time in the past, there may be a snap or click as the shoulder is moved, and the area of the AC joint may become more prominent.
Diagnosis
Usually the diagnosis of AC arthrosis is made during the doctor’s physical examination. In the course of the examination, the doctor will look for tenderness over the AC joint and the presence of pain with compression of the joint. The doctor may determine that an injection of a local anesthetic, such as lidocaine, is indicated. The injection will reduce the pain temporarily and confirm the diagnosis. X-rays may be used to reveal a narrowing of the joint and presence of bone spurs around the joint.
Non-surgical treatment
The goal of treatment for AC arthrosis is to eliminate pain and restore movement to the shoulder. Treatment, initially, may be conservative, consisting of rest and non-steroidal anti-inflammatory medications such as aspirin, ibuprofen, and naproxen. Ice may be applied intermittently as needed to decrease the pain and inflammation at the joint. Cortisone, an anti-inflammatory steroidal medication, may be injected into the joint if the pain persists after the administration of non-steroidal medications. In order to avoid further aggravation of the condition, there should be a lessening of activities that tend to put undue stress on the shoulder.
Surgical treatment
Should rest, ice, medication, and modifying activities not work to reduce the pain and swelling, acromioclavicular joint surgery may be the next step in treatment. The most common procedure for surgically treating AC joint arthrosis is AC joint decompression. In this procedure, the doctor removes approximately 0.5 cm of the end of the collarbone and smooths the worn surfaces at the ends of the AC joint. The major ligaments are kept intact. Scar tissue develops at the decompression site to serve as a cushion pad for the widened joint and allows movement to occur without further abrasion of the ends of the arthritic joint. This procedure maintains the flexibility of the AC joint. The surgery can be done either via a small incision or using arthroscopic techniques involving several smaller incisions.
With either surgical technique, recovery and results are similar. Usually one can go home wearing an arm sling the same day as surgery. Stitches are removed after 7-10 days. Motion exercises begin immediately to prevent shoulder stiffness. Complete motion usually returns in 4-6 weeks. Strength tends to return in 8-12 weeks. A full recovery can be expected in approximately 3-4 months.
Results and Risks of Surgery
Most patients achieve a high level of pain relief from the surgery. nearly 95 percent return to their normal routine of activity and sport with few complications. As with any surgical procedure, there are potential risks. The incidence of infection is generally less than 0.5%.
